
The two go into exactly why they believe that what they promote makes the most sense (carnivore vs. vegan) and give us real data. Dr. Chaffee, a well known Doctor who promotes carnivore takes on Dr. Nagra, a Vegan Doctor.
summerizer
Setup and shared ground
- Dr. Nagra enters as a vegan naturopathic doctor in Vancouver with microbiology training, nutrition writing, textbook contribution, plant-based experience, and clinical work around cardiometabolic risk.
- Dr. Chaffee enters as an American MD in Perth with molecular and cellular biology training, long nutrition study, carnivore practice, and clinical use of dietary intervention.
- Both doctors agree that the prevailing Western diet is unhealthy and that processed-food reliance is a major shared problem.
- The host sets a debate format: define the question, let each doctor give a stance, then let them respond to each other.
- The first major question is what humans are biologically and evolutionarily designed to eat.
Evolution, adaptation, and health outcomes
- Dr. Nagra separates evolutionary adaptation from long-term health and says reproductive success does not automatically equal late-life disease protection.
- He uses sickle-cell protection against malaria as the example: a trait can help survival to reproduction while still carrying later cardiovascular risk.
- He says the relevant endpoint is long-term disease and mortality risk, not whether humans can digest or use a given food.
- Dr. Nagra links higher intake of whole grains, vegetables, fruits, nuts, and legumes with lower all-cause mortality in prospective data.
- He uses enterolactone biomarkers as an intake marker for lignan-rich foods and links higher levels with lower all-cause and cardiovascular mortality.
- He uses the Lyon Diet Heart Study as randomized long-term support for a Mediterranean-style pattern with more bread, fruit, margarine, and less butter, cream, meat, and deli foods.
- Dr. Chaffee says the biological starting point matters because long adaptation to a food group makes harm from that food group unlikely.
- He says wild animals become sick when fed outside their natural diet, and he uses zoos, parks, veterinary medicine, and livestock feeding as analogies.
- He links human evolution with meat dependence, large-animal hunting, ice-age survival, and high human trophic level.
- He says average life expectancy at birth underrates ancestral longevity because infant and child mortality distort the average.
- Their central disagreement is whether diet should start from evolutionary design or measured long-term health outcomes in modern humans.
Vegetables, cohorts, and study interpretation
- Dr. Chaffee uses a UK vegetable-intake paper as an example of mixed nutrition literature and confounding.
- Dr. Nagra checks the table and says fully adjusted all-cause mortality was lower with cooked, raw, and total vegetable intake.
- Dr. Chaffee clarifies that he was focused on cardiovascular risk, not all-cause mortality.
- Dr. Nagra says the study still showed benefit for all-cause mortality and therefore should not be used as a simple no-benefit example.
- Dr. Chaffee says comparisons against the standard diet are limited because both sides already see the standard diet as poor.
- Dr. Nagra answers that swap models do not only compare plant foods with a standard Western diet; they model moving calories or protein from red meat to plant sources.
- Dr. Nagra uses dairy, nuts, legumes, and plant protein swaps as evidence for lower cardiovascular or mortality risk when unprocessed red meat is reduced.
- Dr. Chaffee says each paper needs methodological review and that population averages can conflict with repeated clinical outcomes.
Carnivore survey, selection bias, and calcium scans
- Dr. Chaffee uses the Harvard carnivore survey as evidence that adults on a carnivore diet self-tell improved health.
- Dr. Nagra says the survey recruited from carnivore communities and therefore has strong selection bias.
- Dr. Nagra focuses on coronary artery calcium in people with before-and-after scans and says the score rose from 55 before diet to 81 after or current diet.
- Dr. Nagra says accepting only favorable self-told outcomes while ignoring unfavorable scan data is not a complete use of the paper.
- Dr. Chaffee answers that self-told clinical improvement still matters when many severe conditions reverse in practice.
- The survey becomes a recurring test case for what kind of evidence counts: subjective improvement, objective scans, cohort risk, or patient-level clinical change.
Zoo animals, cancer, and species-appropriate diet
- Dr. Chaffee says animals fed species-appropriate diets in zoos rarely develop diseases such as diabetes, autoimmune disease, cancer, or cardiovascular disease.
- Dr. Nagra answers with zoo-mammal cancer data and says carnivores had the highest cancer mortality among the animal categories he shows.
- Dr. Nagra also raises arthritis and cross-species disease patterns as problems for a simple species-appropriate-diet explanation.
- Dr. Chaffee says animal categories and causes of disease are complex and that the key human issue remains whether humans are adapted to heavy meat intake.
- The exchange tests whether animal feeding analogies can be mapped onto human chronic disease.
Plant-based adequacy, B12, and supplementation
- Dr. Nagra accepts that an unsupplemented and unfortified plant-only diet is not nutritionally complete because vitamin B12 must come from supplements or fortified foods.
- He says a supplemented or fortified plant-based diet can yield nutrient status comparable with omnivores in real populations.
- Dr. Chaffee says a diet needing supplementation is unlikely to be the ancestral human diet.
- Dr. Nagra separates ancestry from adequacy and says modern tools can make a diet workable even when ancestral humans did not eat that way.
- Dr. Chaffee raises B12, heme iron, carnitine, taurine, EPA, DHA, vitamin A, vitamin K2, iodine, zinc, and bioavailability as concerns.
- Dr. Nagra answers that supplementation, fortified foods, K1 conversion, MK7 from natto, beta-carotene conversion, and careful food choice can cover many of those concerns.
- Dr. Chaffee remains focused on whether a diet built from whole animal foods avoids the need for supplementation and conversion uncertainty.
Protein, muscle, and athletic performance
- Dr. Chaffee says animal protein is complete, bioavailable, and naturally packaged with fat-soluble nutrients and fatty acids.
- Dr. Nagra uses protein-matched studies to say plant-based diets can support similar gains in strength and hypertrophy when total protein is adequate.
- Soy isolate, whey, mycoprotein, high-protein vegan diets, and resistance training enter as examples where the total protein dose is controlled.
- Dr. Chaffee questions whether short-term performance and hypertrophy trials settle long-term nutrition quality.
- Dr. Nagra says plant proteins can work in practice when intake and planning are sufficient.
- The disagreement is not only about protein grams; it is also about bioavailability, nutrient package, long-term outcomes, and how much planning is acceptable.
Fiber, diverticular disease, and gut conditions
- Dr. Chaffee challenges common advice around fiber and diverticular disease and says some recommendations historically warned against seeds and fiber.
- Dr. Nagra says current practice in his setting recommends fiber for diverticular disease and gut health.
- Dr. Chaffee says patients with Crohn’s, ulcerative colitis, diverticulitis, and related gut problems can improve when plants are removed.
- Dr. Nagra says observational evidence should not be called causal but still needs direct critique if it is used in the debate.
- The gut section becomes a broader clash between clinical elimination results and population-level fiber data.
Anecdotes, clinical reversals, and causal weight
- Dr. Chaffee says his own health improved when he moved away from plant-heavy eating and toward fatty meat.
- He says patients with Crohn’s, ulcerative colitis, rheumatoid arthritis, MS, lupus, Hashimoto’s, diabetes, insulin resistance, high CRP, high leptin, and dementia-like decline improve on meat-only or meat-centered diets.
- Dr. Nagra says anecdotes run both directions, including carnivore failures, plant reintroductions, vegan improvements, and non-diet examples.
- Dr. Nagra uses smoking with Parkinson’s disease or ulcerative colitis as an example where symptom or risk patterns do not make a behavior broadly healthy.
- Dr. Chaffee says repeated elimination and reintroduction effects in patients function like experiment-like evidence when the same disease patterns improve.
- Dr. Nagra says personal stories are not enough to override long-term disease-risk evidence.
- Dr. Chaffee says population evidence should not erase visible patient recovery when severe symptoms stop.
Plants, toxins, and preparation
- Dr. Chaffee says plants defend themselves chemically and that indiscriminate plant eating can cause harm.
- He uses lectins, kidney beans, oxalates, rhubarb, spinach, animal-husbandry examples, and traditional preparation practices as support.
- Dr. Nagra accepts that some plants need preparation but says ordinary soaking, boiling, pressure cooking, and food practices usually reduce the risk.
- Dr. Nagra uses the white kidney bean incident as an example of acute illness from improper preparation, not proof that all beans are unsafe.
- Dr. Chaffee says plant toxins are not imaginary and that processing traditions exist for a reason.
- Dr. Nagra says animal foods also require preparation and carry contamination risk.
Foodborne illness and contamination
- Dr. Nagra contrasts lectin-poisoning incidents with Salmonella and E. coli burdens from animal foods.
- He gives annual Salmonella figures of 1.35 million infections, 26,500 hospitalizations, and 420 deaths in the United States.
- He says a portion of Salmonella burden is attributable to chicken and turkey.
- He also uses E. coli outbreak attribution to ground beef as a counterpoint to plant-toxin concern.
- Dr. Chaffee answers that foodborne contamination and intrinsic plant toxins are different categories of risk.
- The shared practical point is that both plant and animal foods can be harmful when selection, storage, or preparation fails.
Traditional populations and historical diet comparisons
- Dr. Chaffee uses the Maasai and Kikuyu comparison to support the view that the higher-meat pastoral population had greater stature, strength, and health markers.
- Dr. Nagra says the Kikuyu pattern in that old comparison was low-protein, low-fat, low-calcium, and not a modern well-planned plant-based diet.
- Dr. Chaffee says a whole civilization living generationally on a plant-heavy diet is still relevant evidence if health markers were worse.
- Dr. Nagra raises confounders such as genetics, hospital access, disease environment, life expectancy, and cardiovascular endpoints.
- Dr. Chaffee also points to Plains Indians, Inuit diet history, and ice-age hunting as evidence for meat-centered human adaptation.
- Dr. Nagra points to Greenland Inuit mummies, Egyptian mummies, Lithuanian mummies, and Maasai autopsy material as evidence that atherosclerosis can occur in traditional or high-animal-food settings.
- Dr. Chaffee answers that atherosclerosis has many possible causes, including stress, smoking, infection, and other exposures.
Closing split
- Dr. Nagra closes on outcome evidence: higher intake of healthful plant foods, especially when replacing meat, aligns with lower cardiometabolic, diabetes, cancer, and mortality risk.
- Dr. Chaffee closes on biology and clinical response: humans are meat-adapted, severe disease often improves on carnivore, and studies that conflict with repeated patient outcomes deserve skepticism.
- Both sides agree that processed food is a core problem.
- They remain split on whether plant-forward long-term outcome data or carnivore evolutionary logic is the stronger guide.
- The debate also remains split on what evidence has priority: cohorts, trials, biomarkers, mechanistic biology, ancestral reconstruction, objective scans, or clinical reversals.
References
- [00:06] Food groups and risk of all-cause mortality: a systematic review and meta-analysis of prospective studies — https://doi.org/10.3945/ajcn.117.153148
- [00:07] Association of Polyphenol Biomarkers with Cardiovascular Disease and Mortality Risk: A Systematic Review and Meta-Analysis of Observational Studies — https://doi.org/10.3390/nu9040415
- [00:07] Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study — https://doi.org/10.1161/01.CIR.99.6.779
- [00:11] The evolution of the human trophic level during the Pleistocene — https://doi.org/10.1002/ajpa.24247
- [00:22] Behavioral Characteristics and Self-Reported Health Status among 2029 Adults Consuming a “Carnivore Diet” — https://doi.org/10.1093/cdn/nzab133
- [00:24] Association Between Plant and Animal Protein Intake and Overall and Cause-Specific Mortality — https://doi.org/10.1001/jamainternmed.2020.2790
- [00:27] Red meat intake and risk of coronary heart disease among US men: prospective cohort study — https://doi.org/10.1136/bmj.m4141
- [00:35] Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland — https://doi.org/10.1007/s00394-015-1079-7
- [01:00] High-Protein Plant-Based Diet Versus a Protein-Matched Omnivorous Diet to Support Resistance Training Adaptations: A Comparison Between Habitual Vegans and Omnivores — https://doi.org/10.1007/s40279-021-01434-9
- [01:21] Total Meat Intake is Associated with Life Expectancy: A Cross-Sectional Data Analysis of 175 Contemporary Populations — https://doi.org/10.2147/IJGM.S333004
- [01:22] Nutrition and Health - The Association between Eating Behavior and Various Health Parameters: A Matched Sample Study — https://doi.org/10.1371/journal.pone.0088278
- [01:25] Vegan and Omnivorous High Protein Diets Support Comparable Daily Myofibrillar Protein Synthesis Rates and Skeletal Muscle Hypertrophy in Young Adults — https://doi.org/10.1016/j.tjnut.2023.02.023
- [01:31] Red kidney bean poisoning in the UK: an analysis of 50 suspected incidents between 1976 and 1989 — https://pmc.ncbi.nlm.nih.gov/articles/PMC2271815/
- [01:51] Studies of Nutrition: The Physique and Health of Two African Tribes — https://babel.hathitrust.org/cgi/pt?id=coo.31924003510108
- [02:01] Atherosclerosis in 16th-Century Greenlandic Inuit Mummies — https://doi.org/10.1001/jamanetworkopen.2019.18270
- [02:04] Evaluating agreement between bodies of evidence from randomised controlled trials and cohort studies in nutrition research: meta-epidemiological study — https://doi.org/10.1136/bmj.n1864
- [02:04] Evaluating concordance of bodies of evidence from randomized controlled trials, dietary intake, and biomarkers of intake in cohort studies: a meta-epidemiological study — https://doi.org/10.1093/advances/nmab095
You must log in or # to comment.
I typically try to avoid posting direct VS content on other lifestyles, but recently I had a few interactions where someone was so emotionally angry they were unable to have a discussion about their points - to the level of flat out refusing to “platform/debate a carnist”…
Given I can’t have the organic discussion with real humans, let’s look at two medical doctors have that back and forth for us.
Notice the energy and stress vs calmness of the two doctors when the discussion gets heated.
deleted by creator
I’ve spoken on how I critically read papers before - https://discuss.online/post/25820268
Here is a generated infographic from that
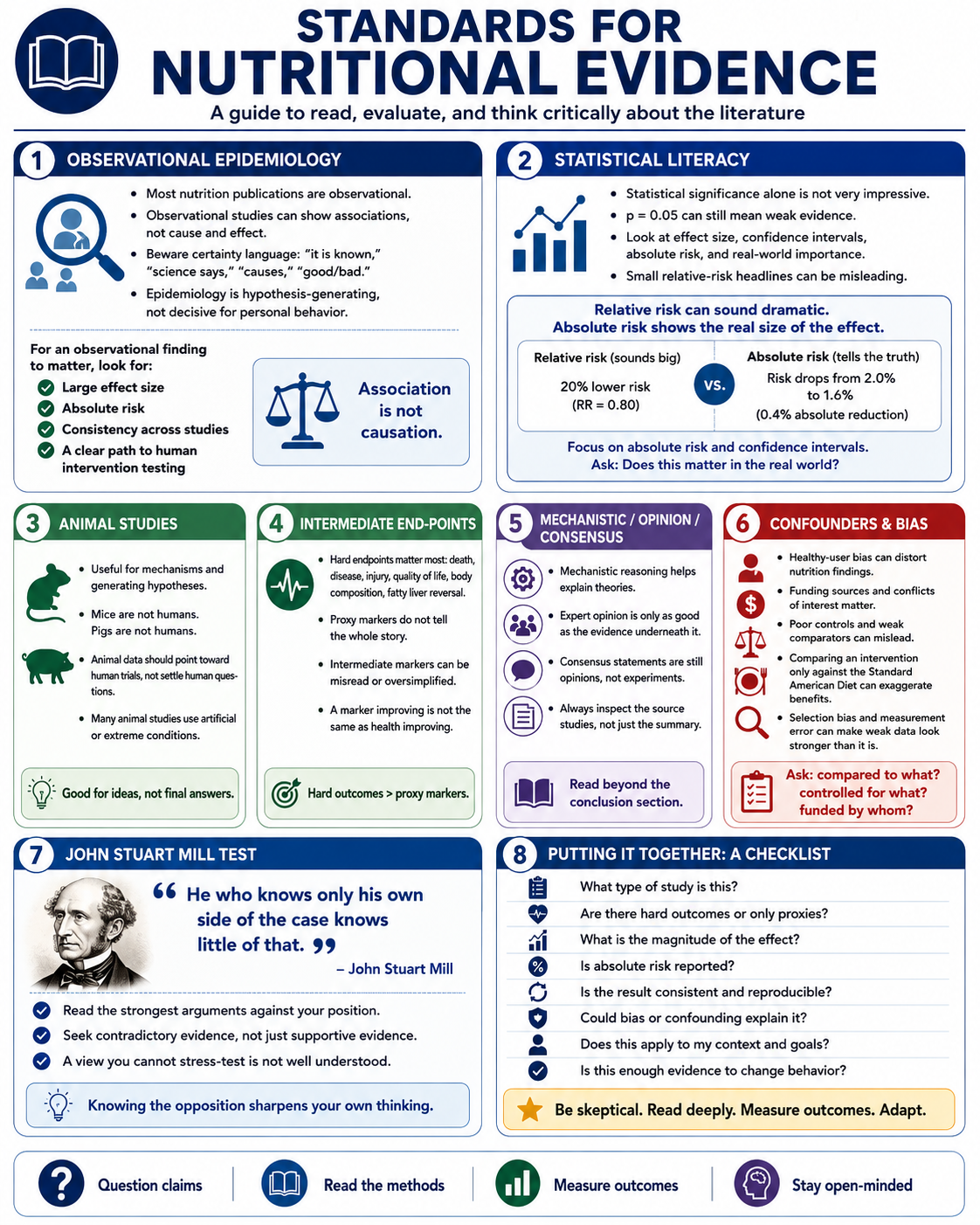
One big schism in this debate is where the two doctors fall on the causal claims of epidemiology , I dare say one of the doctors is not applying a uniform evidentiary standard to the papers they are citing…
At the end did either doctor change their mind? No, because the real issue here isn’t plant vs animal, its their different standards of evidence they use to make decisions.
deleted by creator
I live near a forest with clean spring water and my B12 levels are normal on a wfpb diet without supplements.
How frequently do you do a blood test?
deleted by creator